
What's Holding Up New Long Term Care Beds?
Stop blaming staffing shortages

Hospital emergency department and surgery wait times across Canada are a disaster. One significant reason for that is a backlog of “corridor patients” waiting to be admitted to the hospital itself.1
Admissions are backlogged because there aren’t enough beds available.
Beds are often in short supply because they’re being occupied by Alternate Level of Care (ALC) patients - who no longer need acute hospital care but remain in hospital beds because there’s nowhere appropriate to discharge them.
ALC patients are often stuck where they are because there aren’t enough Long Term Care (LTC) beds available.
And LTC beds are in short supply because…well, just why are they in short supply? A lot of the story revolves around negative incentives that can convince investors to avoid the market altogether.
Rising construction and borrowing costs are certainly a factor. It’s estimated that a modern LTC facility often costs $300k–$400k per bed to build in Canada.
Delays due to the usual licensing, permitting, and plain old government inertia issues play a role. It can take close to a decade from an official announcement of a new public LTC facility before a facility opens.
Regulatory inflexibility can limit the ability of providers to adjust their pricing to account for economic changes.
Finding trained staff to handle the huge growth in demand is, according to some analyses, the most significant problem.
Let’s take a closer look at staffing. According to Statistics Canada, there were 282,818 individuals employed by nursing and residential care facilities in 2003. By 2024, that number had risen 83 percent to 516,898.
Of course, because the patient population could have grown even faster over that time, that number won’t help us. Unfortunately there’s no useful data available representing the number of patients in residential care over time. So we’ll have to look for proxies.
Canada’s population grew by 30 percent through those 21 years. Using the annual population numbers we can calculate that the number of nursing and residential care facilities employees per 1,000 Canadians grew from 8.87 to 12.53. That’s a relative growth rate of 40 percent, which is significantly faster than the overall population change. If that’s the whole story, than there should be no staffing shortages in the industry.
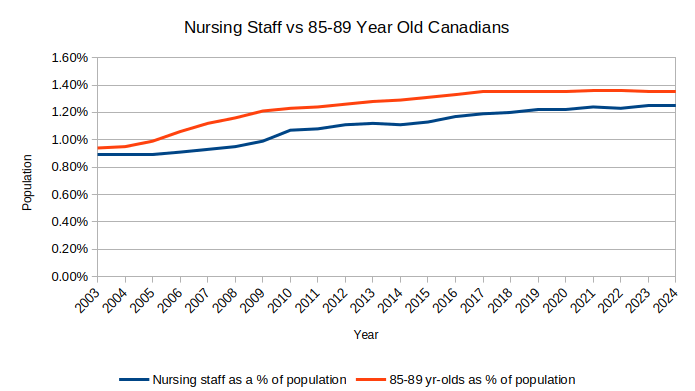
Of course, since we all know that Canada’s elderly make up a rising proportion of the population, we should probably narrow down our focus. In 2003, Canadians aged 85-89 made up 0.94 percent of the total population. That number had grown to 1.35 percent by 2024. The change was just over 44 percent.
As you can see from the chart below, the elderly population (the people most likely to require residential care) is growing faster than the cohort of caregivers they need - but not much faster. The relatively narrow difference isn’t nearly enough to fully explain the depth of the shortage in beds.
Assuming this official data is accurate, claims that workers abandoned the industry in large numbers during and after COVID are simply wrong.
It’s unlikely that the patient-caregiver ratio has increased over the past decades. If anything, the spread of labour-saving tools like patient lift devices and electronic monitoring has probably reduced the proportional staffing needs. And while competition from higher-paying hospital jobs has always been a challenge, hourly wages for the sector have actually more than kept pace with inflation.
To some degree there isn’t any simple solution to the LTC supply problem - and, by extension, to the consequent problems with healthcare access in general. But there are definitely opportunities for partial wins, especially when it comes to government’s traditional role as a provider of artificial constraints.
Or, to put it differently, it would be wonderful if Canadian governments at all levels rediscovered the fine art of getting out of the way of people who want to build stuff.
Other contributing causes include the lack of available emergency clinical staff, the fact that conditions that could be treated in the community by primary providers are missed because millions of Canadians can’t find primary physicians, and recent uncontrolled growth of the general population.
It is a trivial matter, but your chart is labelled "85 to 59" when it means "85 to 89".
You’ve identified the conundrum. For the want of sufficient LTC beds, patients wait too long in emergency departments, and some of those die. It’s a variation of the proverb about “for want of a nail, the kingdom was lost”.
The government approach to LTC is typical government stuff. It’s expensive, the need seems to be insatiable, and so they ration it. Rationing doesn’t remove the demand for the care, however. People get old and infirm, and some need a lot of care. Needing LTC is the final common pathway for a lot of diseases, in fact for aging itself. Most of the time, it’s personal care (bathing, dressing, feeding, and safe-keeping), rather than skilled nursing care.
There was a notion that people could “age in place”, given adequate supports, and a hope that the home care approach would be cheaper. To that end, much effort goes into ensuring that home care options have been exhausted before LTC options are considered. All that assessment takes time and consumes resources. When the home care options fail, however, as when a frail older person falls at home and breaks a hip, then the person ends up in hospital, where, having been proven to no longer qualify for home care, they await LTC. There’s no quick path from failed home care to LTC that skips the hospital.
Feeling that some people were exploiting the hospital route to LTC admission, many governments refuse to prioritize hospital inpatients for LTC admission, which means that everybody democratically waits an equally long time to get into LTC, even the ones clogging up expensive hospital beds. Further assessments are done, committees decide who gets into nursing homes. This is a waste of time and resources, and harmful to others needing hospital care.
It’s also become a fact that many of those who get into LTC have been on the decline for a long time, so they are nearing the end of life. The average life span for a new admission to LTC here in Nova Scotia is now, as a result, just over a year. You wait months to get into a bed you’ll probably occupy for less than a year! Once you’ve died, your room gets cleaned and sanitized (after your family clean out your belongings), and then the bed is declared available, whereupon a process begins to select the next fortunate occupant. This takes a few weeks, during which the bed sits empty!
As it’s partially government funded (patients are often expected to chip in for their own “room and board” costs, as their finances allow, part of the assessment process involves looking at your finances, as well as your care needs. More bureaucracy!
Finally, you can’t build a nursing home without government permission. As with schools, this leaves them perpetually behind, reactive rather than proactive.
In short, it’s a highly bureaucratic system, much of the (expensive) bureaucracy being there to control costs. Like many things, it probably would work better with the government out of the way.